


How early is early when it comes to preventing dementia?
We have to start our #BrainHealth, #HeartHealth and #MetabolicHealth messages and lifestyle changes when we are young if we want to maintain our biological resilience.

For those of us who work in, or think about, preventive medicine, it is obvious that you have to act early to have an impact further down the line. It is clear that human biology is like a network that has many interconnected nodes. Our biological network maintains resilience, which ultimately protects you from the ravages of ageing and the inevitable cognitive decline that will happen to the vast majority of us if we live long enough. Therefore we need to maintain this network as best we can when we are young. If we take out one of the nodes of the network or weaken its connections with disease then we reduce its future resilience and ability to buffer cognitive decline.

I am not surprised that multimorbidity is a risk factor for dementia. In the prospective 30 year follow-up of the Whitehall II study multimorbidity, particularly when the onset is in midlife rather than late life, is strongly associated with subsequent dementia. The message is loud and clear we have to start our #BrainHealth, #HeartHealth and #MetabolicHealth messages and lifestyle changes when we are young if we want to maintain our biological resilience to protect ourselves from getting dementia.
Please don’t forget the Whitehall studies have been heavily criticised for being quite selective in terms of their demographic profile (male, white and highly-educated) and hence the signal seen in this study may be much larger in the general population.
Whatever your age dare I suggest you stop and reflect on your brain, heart and metabolic health and ask what you need to do to optimise them so as to reduce your chances of getting dementia as you age.
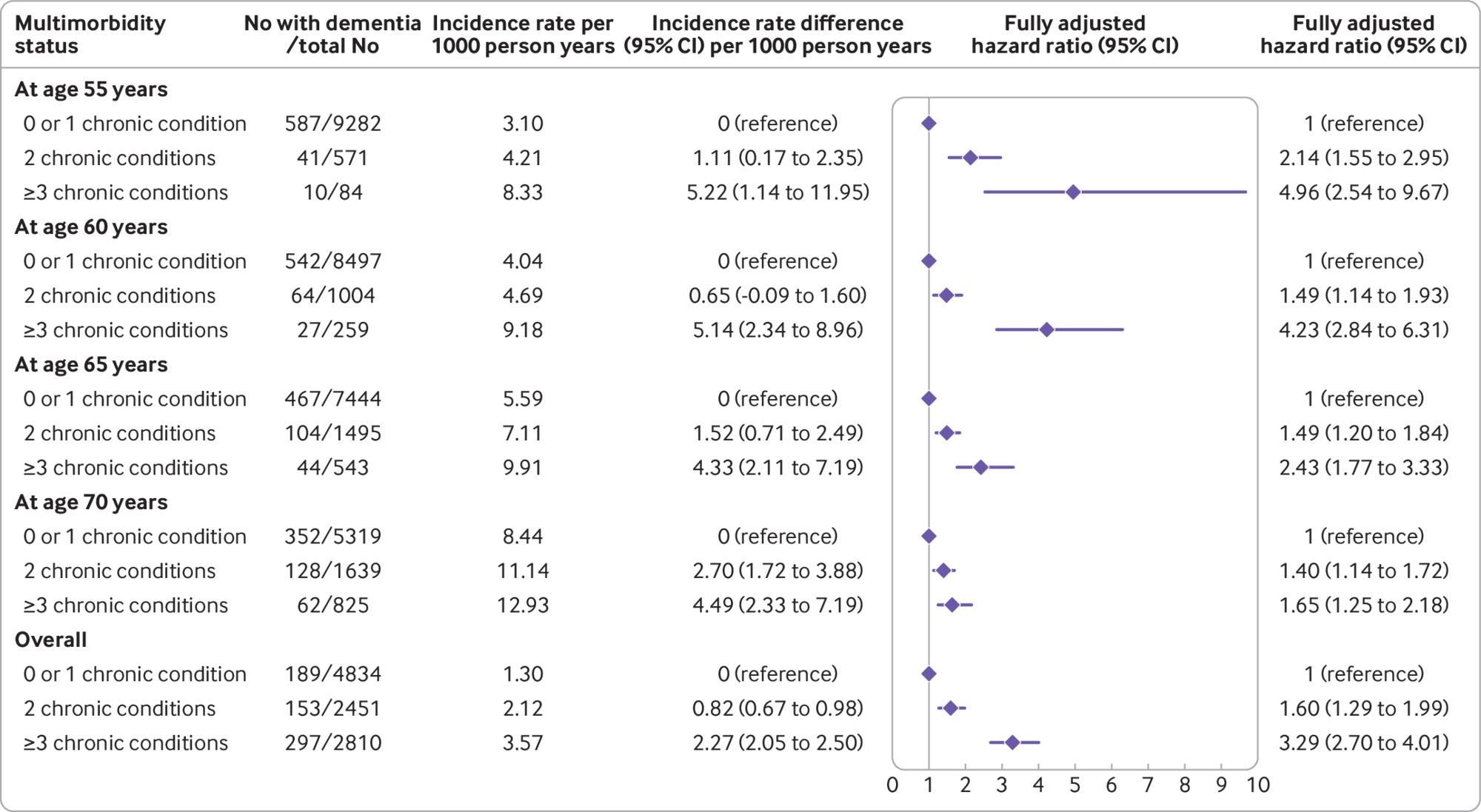
Figure: Association between the number of chronic conditions (≤1, 2, and ≥3) and subsequent risk of dementia. Chronic conditions considered were coronary heart disease, stroke, heart failure, diabetes, hypertension, cancer, chronic kidney disease, chronic obstructive pulmonary disease, liver disease, depression, mental disorders, Parkinson’s disease, and arthritis/rheumatoid arthritis. Analyses were stratified on the birth cohort (5-year groups) and adjusted for age (as time scale), sex, ethnicity, education, marital status, and health behaviours (smoking, alcohol consumption, physical activity, and diet). Covariates measurement was concurrent with the measure of multimorbidity
Objective: To examine the association of midlife and late-life multimorbidity, including the severity of multimorbidity, with incident dementia.
Design: Prospective cohort study.
Setting: Civil service departments in London (Whitehall II study, study inception in 1985-88).
Participants: 10 095 participants, aged 35 to 55 at baseline.
Main outcome measure: Incident dementia at follow-up between 1985 and 2019. Cause-specific Cox proportional hazards regression was used to examine the association of multimorbidity overall and at age 55, 60, 65, and 70 with subsequent dementia taking into account the competing risk of death.
Results: The prevalence of multimorbidity (≥2 chronic diseases) was 6.6% (655/9937) at age 55 and 31.7% (2464/7783) at age 70; 639 cases of incident dementia occurred over a median follow-up of 31.7 years. After adjustment for sociodemographic factors and health behaviours, multimorbidity at age 55 was associated with subsequent risk of dementia (difference in incidence rate per 1000 person-years 1.56, 95% confidence interval 0.62 to 2.77; hazard ratio 2.44, 95% confidence interval 1.82 to 3.26). The association weakened progressively with older age at onset of multimorbidity. At age 65, onset of multimorbidity before age 55 was associated with 3.86 (1.80 to 6.52) per 1000 person-years higher incidence of dementia (hazard ratio 2.46, 1.80 to 2.26) and onset between 60 and 65 was associated with 1.85 (0.64 to 3.39) per 1000 person-years higher incidence (1.51, 1.16 to 1.97). Severity of multimorbidity (≥3 chronic diseases) at age 55 was associated with a 5.22 (1.14 to 11.95) per 1000 person-years higher incidence of dementia (hazard ratio 4.96, 2.54 to 9.67); the same analyses at age 70 showed 4.49 (2.33 to 7.19) per 1000 person-years higher incidence (1.65, 1.25 to 2.18).
Conclusion: Multimorbidity, particularly when onset is in midlife rather than late life, has a robust association with subsequent dementia. The increasingly younger age at onset of multimorbidity makes prevention of multimorbidity in people with a first chronic disease important.
MS Research MS-Selfie Newsletter
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.