

Preventable Traumatic Brain Injury in Rugby Players
Preventable Traumatic Brain Injury in Rugby Players
Repeated minor head injuries are associated with evidence of axonal injury and reduced brain reserve in professional rugby players.

Head injuries, particularly recurrent head injuries, are a well-defined risk factor for all-cause dementia. The question we need to ask is, ‘are head injuries preventable?’.

In this longitudinal observational study in professional male and female rugby players there was clear neuroimaging evidence of axonal injury or diffuse vascular injury in a quarter of players. In contrast, non-collision-sport athletic controls did not show these abnormalities.
Alarmingly longitudinal imaging revealed reductions in brain volume (white matter) in the elite rugby players studied. These changes were not related to self-reported head injury history or neuropsychological test scores. The latter may simply be due to the relatively small size of the study or possibly due to compensatory mechanisms that allow the damaged brain to compensate whilst there is sufficient reserve capacity present.
This study supports data from other contact sports (boxing, outfield football/soccer players, American football, ice hockey, etc.) that repeated head injuries come with a cost to the brain. Repeated minor head injuries are associated with evidence of axonal injury and reduced brain reserve. Applying the well-established principle of brain health that reduced brain reserve is a risk factor for all-cause dementia it is highly likely that professional rugby players are at greater risk of developing all-cause dementia in the future and potentially other common neurodegenerative diseases.
What is not clear from this study is whether or not the brain damage suffered by repeated rugby-related head injuries is sufficient to cause chronic traumatic encephalopathy (CTE) that has been described in American football players.
I suspect this study which is supported by data on biomarkers of neuronal damage (second study below) will have major repercussions for both professional and amateur rugby. How will the different rugby codes address this issue? It is unlikely any rule changes will be able to eliminate the risk of head injuries in contact sports. I suspect many parents may want to discourage their children from playing rugby and other contact sports after reading this paper. Is the data definitive enough to run a public health campaign? Allyson Pollock, a Professor of Public Health at Newcastle University, has been running a campaign against school rugby for over a decade and has written a book on the subject for parents.
“Tackling Rugby: What Every Parent Should Know” by Allyson M. Pollock.
What would my advice be to a professional rugby player with this knowledge? I suspect most professional rugby players have known about the risk for some time; this will be based on the shitstorm that erupted in the US over CTE in American football players.
Rugby is a gladiatorial sport therefore knowing what risks rugby players are taking with their brains may make the sport more, not less, appealing. If you want to age well, i.e. with a healthy brain, would you play a contact sport? Sport, including contact sports, make life interesting and more enjoyable and many people will therefore take their chances and ignore the health messages on head injury prevention.
I am confident this issue has legs and will run for some time. There will be many more commentators who will have a different opinion from mine, including the lawyers. Watch this space.
Zimmerman et al. White matter abnormalities in active elite adult rugby players. Brain Communications, Volume 3, Issue 3, 2021, fcab133, https://doi.org/10.1093/braincomms/fcab133
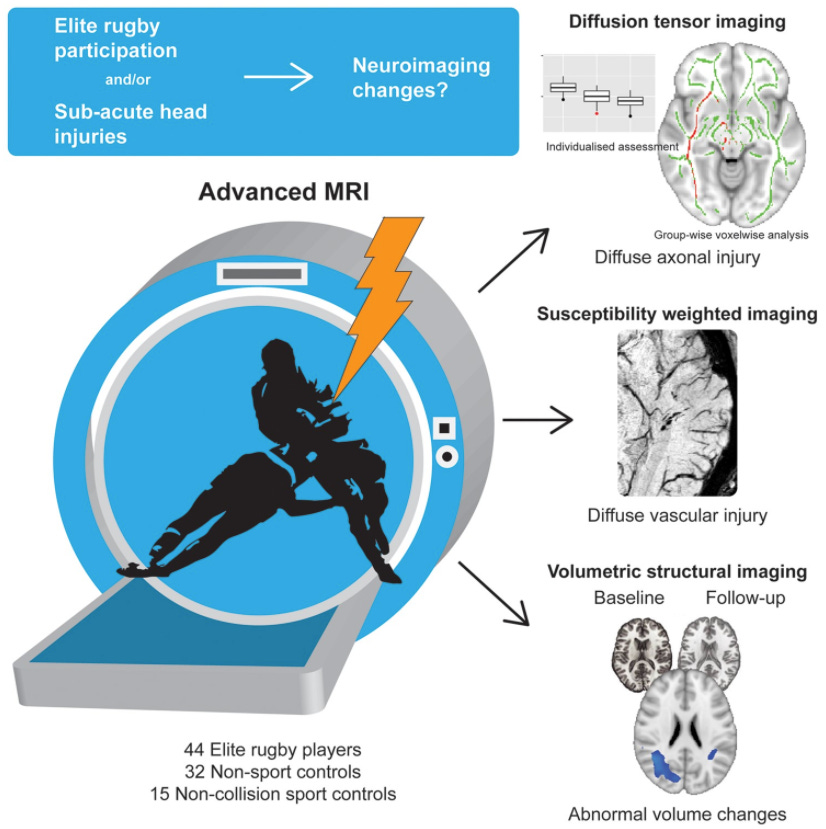
The recognition, diagnosis and management of mild traumatic brain injuries are difficult and confusing. It is unclear how the severity and number of injuries sustained relate to brain injuries, such as diffuse axonal injury, diffuse vascular injury and progressive neurodegeneration. Advances in neuroimaging techniques enable the investigation of neuropathologies associated with acute and long-term effects of injury. Head injuries are the most commonly reported injury seen during professional rugby. There is increased vigilance for the immediate effects of these injuries in matches, but there has been surprisingly little research investigating the longer-term effects of rugby participation. Here, we present a longitudinal observational study investigating the relationship of exposure to rugby participation and sub-acute head injuries in professional adult male and female rugby union and league players using advanced MRI. Diffusion tensor imaging and susceptibility weighted imaging was used to assess white matter structure and evidence of axonal and diffuse vascular injury. We also studied changes in brain structure over time using Jacobian Determinant statistics extracted from serial volumetric imaging. We tested 41 male and 3 female adult elite rugby players, of whom 21 attended study visits after a head injury, alongside 32 non-sporting controls, 15 non-collision-sport athletic controls and 16 longitudinally assessed controls. Eighteen rugby players participated in the longitudinal arm of the study, with a second visit at least 6 months after their first scan. Neuroimaging evidence of either axonal injury or diffuse vascular injury was present in 23% (10/44) of players. In the non-acutely injured group of rugby players, abnormalities of fractional anisotropy and other diffusion measures were seen. In contrast, non-collision-sport athletic controls were not classified as showing abnormalities. A group level contrast also showed evidence of sub-acute injury using diffusion tensor imaging in rugby players. Examination of longitudinal imaging revealed unexpected reductions in white matter volume in the elite rugby players studied. These changes were not related to self-reported head injury history or neuropsychological test scores and might indicate excess neurodegeneration in white matter tracts affected by injury. Taken together, our findings suggest an association of participation in elite adult rugby with changes in brain structure. Further well-designed large-scale studies are needed to understand the impact of both repeated sports-related head impacts and head injuries on brain structure, and to clarify whether the abnormalities we have observed are related to an increased risk of neurodegenerative disease and impaired neurocognitive function following elite rugby participation.
Laverse et al. Plasma glial fibrillary acidic protein and neurofilament light chain, but not tau, are biomarkers of sports-related mild traumatic brain injury. Brain Commun. 2020 Sep 7;2(2):fcaa137.
Mild traumatic brain injury is a relatively common event in contact sports and there is increasing interest in the long-term neurocognitive effects. The diagnosis largely relies on symptom reporting and there is a need for objective tools to aid diagnosis and prognosis. There are recent reports that blood biomarkers could potentially help triage patients with suspected injury and normal CT findings. We have measured plasma concentrations of glial and neuronal proteins and explored their potential in the assessment of mild traumatic brain injury in contact sport. We recruited a prospective cohort of active male rugby players, who had pre-season baseline plasma sampling. From this prospective cohort, we recruited 25 players diagnosed with mild traumatic brain injury. We sampled post-match rugby players without head injuries as post-match controls. We measured plasma neurofilament light chain, tau and glial fibrillary acidic protein levels using ultrasensitive single molecule array technology. The data were analysed at the group and individual player level. Plasma glial fibrillary acidic protein concentration was significantly increased 1-h post-injury in mild traumatic brain injury cases compared to the non-injured group (P = 0.017). Pairwise comparison also showed that glial fibrillary acidic protein levels were higher in players after a head injury in comparison to their pre-season levels at both 1-h and 3- to 10-day post-injury time points (P = 0.039 and 0.040, respectively). There was also an increase in neurofilament light chain concentration in brain injury cases compared to the pre-season levels within the same individual at both time points (P = 0.023 and 0.002, respectively). Tau was elevated in both the non-injured control group and the 1-h post-injury group compared to pre-season levels (P = 0.007 and 0.015, respectively). Furthermore, receiver operating characteristic analysis showed that glial fibrillary acidic protein and neurofilament light chain can separate head injury cases from control players. The highest diagnostic power was detected when biomarkers were combined in differentiating 1-h post-match control players from 1-h post-head injury players (area under curve 0.90, 95% confidence interval 0.79-1.00, P < 0.0002). The brain astrocytic marker glial fibrillary acidic protein is elevated in blood 1 h after mild traumatic brain injury and in combination with neurofilament light chain displayed the potential as a reliable biomarker for brain injury evaluation. Plasma total tau is elevated following competitive rugby with and without a head injury, perhaps related to peripheral nerve trauma and therefore total tau does not appear to be suitable as a blood biomarker.
Conflicts of Interest: I sit on the oversight committee that provided advice on this TBI study.
MS Research MS-Selfie Newsletter
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of the Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust and are not meant to be interpreted as personal clinical advice.