


Can we predict MS?
Pipedreams and possibilities

COI: Ben is a researcher working on the ADAMS study - https://app.mantal.co.uk/adams - a genetics study aiming to understand how genes influence MS risk across different ancestral backgrounds.
Preventing Multiple Sclerosis is the long-term goal for our research group and for many other researchers worldwide. It is also a key research priority for many people with MS. It’s a very ambitious goal and while I am optimistic we will see advances in this area in the coming decades, we’re a very long way off being able to prevent MS.
A central reason that preventing MS is so challenging is that it requires two things which we don’t currently have:
An effective means of prevention (this could be for instance an EBV vaccine, high-dose vitamin D, or something else), and
An accurate understanding of who should be offered this means of prevention.
The flurry of recent discoveries about the role of EBV in MS has given many people hope - if EBV really does cause MS, it’s possible an EBV vaccine may be able to prevent MS in some people. Perhaps this will be an effective means of prevention, perhaps not. We need trials to see.
A less obvious but equally tricky problem is who should be offered this kind of preventive therapy. Before a preventive measure is rolled out en masse, we need trial data to prove that it works. But proving that it works is a challenge with a relatively rare disease like MS. If about 1 in 500 people get MS in the general population, and a hypothetical EBV vaccine reduces the risk of MS by 10%, you would need a massive trial to prove an effect. Here’s a graph showing how many people you would need in this kind of study. The x axis shows different degrees of effectiveness of a possible vaccine, and the y axis shows how many people you would need in each arm of the study to see an effect:
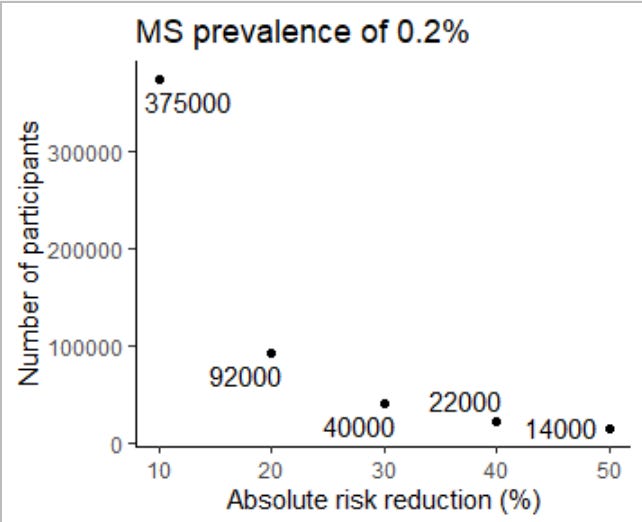
Even for a very effective vaccine (reducing your risk of MS by 50%), you would still need to find 28,000 people in total (14,000 for the vaccine, 14,000 for placebo). This would take vast amounts of money and time, and would incur a substantial opportunity cost if it didn’t work - that’s money and time that could be spent on other MS research, improving services, or improving access to treatment.
But what if we had an effective way of predicting who was at higher risk of MS? This would allow us to select people at high risk for a prevention trial. If we could find people whose MS risk is 1 in 100, rather than the baseline of 1 in 500, we would be able to do the trial with far fewer people (6,000 in total):

Taking it further, if we could find an even higher-risk group (e.g. a baseline risk of 1 in 20), you could run the trial with 600 participants in each group:

So if we were capable of identifying people at high risk of MS, we would have a much better chance of proving (or definitively disproving) the effectiveness of interventions in preventing MS. And down the line, if it becomes clear that there are effective ways of reducing the risk of MS (e.g. an EBV vaccine), robust predictive risk scores could help work out who is most likely to benefit from such a measure.
That’s why predicting MS is important. But are we anywhere near being able to predict MS reliably?
The short answer is no, in my view. Even with detailed genetic information and information about someone’s exposure to risk factors (e.g. smoking, low vitamin D, glandular fever), we are still nowhere near being able to robustly work out who will get MS and who won’t. There are many reasons for this, including the relative rarity of the disease, our incomplete map of how genetics influences risk, and our poor understanding of how environmental factors increase risk.
One major problem with efforts to make ‘MS risk scores’ is that we have an incomplete understanding of whether MS risk genes have the same effects across different ancestral backgrounds. This is partly because there is a lack of data on genetics and MS risk in non-European populations. The largest genetic study of MS in people of European ancestry had about 50 times the number of participants with MS than the largest study in people of African ancestry. This problem has been recognised across other diseases - attempts to predict a disease in people of non-European ancestry using reference genetic information from people of European-ancestry is woefully inaccurate. MS is no exception. If you’re interested in more detail on this topic, we’ve written a mini-review about why MS risk scores perform so badly in reality. You can read it here for free.
MS prevention studies are hopefully on the horizon. Making them tractable and affordable requires methods for identifying people at high risk of MS. There’s lots of work to be done to improve these methods. We are trying to ensure that efforts to develop MS risk scores do not unfairly exclude people of non-European ancestry from prevention trials. To do so, we’re comparing the DNA of people with MS who identify as having non-European ancestry with people who don’t have MS. If you’d like to find out more about our study - the ADAMS study - take a look at the website or get in touch via email.
Prediction paves the way for prevention, but accurate prediction of MS risk remains a work in progress.
Dr Jacobs, nice post.
But why not do the MS prevention study as part of a national registry study after an EBV vaccine is licensed and offered as part of the national vaccine programme; say for the prevention of infectious mononucleosis? By doing this you can look at the impact of EBV vaccination on not only the incidence of MS, but also on other EBV-associated diseases (cancers, SLE, primary biliary cirrhosis, Sjogren's syndrome, rheumatoid arthritis, etc.)?
I think every individual diagnosed with MS, should be tested their vitamin D levels. I feel very low vitamin D reactivates the EBV. .
Has anyone looked at that. My daughter's vitamin D was 17 nmol on diagnosis and the Neurologist that diagnosed her, did not look into her vitamin D levels.
Her vitamin D levels generally over 110 nmol now,
and her treatment with Mavenclad has been very effective. I will be very interested in Dr G's comment.